Chronic condition ascertainment in Medicare: A pre to post COVID-19 onset comparison
Principal Investigator
RJ Waken, Instructor, Division of Biostatistics, Washington University School of Medicine in St. Louis
Co-Investigators
- Fengxian Wang, Statistical Data Analyst, Washington University School of Medicine in St. Louis
- Karen Joynt-Maddox, Associate Professor, Washington University School of Medicine in St. Louis
Funded By
Social, Behavioral, and Economic COVID Coordinating Center (SBE CCC)
The Problem
Research using claims data relies on accurate ascertainment of chronic conditions (CCs) for cohort identification and risk adjustment. However, during the COVID-19 pandemic, utilization patterns changed as a result of institutional directives and decreased patient care-seeking behavior—which may have affected CC ascertainment.
This study aims to characterize changes over time in comorbidity prevalence to inform researchers of potential shifts in coding patterns when using Medicare claims data for research. Further, the research team seeks to determine whether these patterns differ between feefor-service (FFS) and Medicare Advantage (MA) given known differences in incentives for upcoding.
The Approach
Waken and colleagues recreated Medicare’s Chronic Conditions Warehouse (CCW) algorithms for identifying comorbidities to the day (rather than yearly) using the pre-specified 1 and 2 year look back periods in both FFS and MA claims files.
They then compared the prevalence (in beneficiary days) of each of the 30 derived CCs over time and cross sectionally. Finally, they conducted analyses overall and stratified by FFS vs MA status
The Findings
Between Q1 2019 and 2022, the share of FFS / MA beneficiaries shifted from 63.6% / 36.4% to 55.0% / 45.0%, but many other beneficiary characteristics remained similar (Figure 1).
Fewer CCs were coded overall per beneficiary over time in both MA and FFS (Figure 2).
Examining the CCWs individually, the researchers found the largest drops in stroke, hypertension, and chronic obstructive pulmonary disease. No drop was found in most cancers. Increases were found in hyperlipidemia, chronic kidney disease, and depression. The patterns were similar between MA and FFS, with notable differences in depression, anemia, and heart failure.
These findings indicate that healthcare utilization changes during the COVID-19 pandemic likely drove meaningful changes in CC capture. If these utilization changes do not represent underlying population shifts in illness or disease burden, analyses conditioning inferences on membership in prior utilization-based disease groups, or using CC-based risk adjustment may be subject to bias.
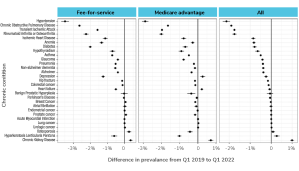
A dot-and-whisker plot showing the difference in prevalence of various chronic conditions (listed along the y-axis) from Q1 2019 to Q1 2022. The x-axis represents the percentage difference in prevalence ranging from -3.0% to 1.0%. The plot is divided into three panels: FFS (Fee-for-Service), MA (Medicare Advantage), and All, representing different beneficiary groups. Each condition (e.g., HTN, COPD, Stroke_TIA, etc.) is shown as a dot with a horizontal line (confidence interval) for each group. Most conditions show a decrease in prevalence over time (dots left of center line), with some variation between FFS and MA groups. HTN (hypertension) shows the largest decrease across all groups, while some conditions (e.g., chronic kidney disease) show a slight increase.