The impact of telehealth on diabetes management in a safety-net health system during the COVID-19 pandemic
Principal Investigator

Cameron Kaplan
Associate Professor, Medicine, Director of the Gehr Family Center for Health Systems Science and Innovation, Keck School of Medicine, University of Southern California
Co-Investigators
- Chun Nok Lam, Research Scientist, Emergency Medicine, University of Southern California
- John Thacker, Research Programmer, Schaeffer Center, University of Southern California
- Todd Schneberk, Assistant Professor, Clinical Emergency Medicine, University of Southern California
- Jennifer Tsui, Associate Professor, Population and Public Health Sciences, University of Southern California
- Sarah Axeen, Director of Data and Analytics, Schaeffer Center; Assistant Professor, Division of Emergency Medicine Research, University of Southern California
Funded By
National Institute on Minority Health and Health Disparities (NIMHD)
The problem:
As the COVID-19 pandemic disrupted healthcare access across the nation, telehealth emerged as an alternative to in-person care. Telehealth served as a stop-gap for many vulnerable populations, including those with diabetes. However, the impact of the use of telehealth on diabetes management remains unclear.
This study examines whether telehealth use influenced A1c testing, glycemic control, and acute care utilization among patients in the Los Angeles County Department of Health Services (LAC DHS) safety-net system.
The approach:
This retrospective cohort study uses LAC DHS encounter data from 2019 to 2021. The researchers identified patients continuously empaneled in the health system from March 2019 to April 2021. The researchers categorized patients based on their exposure to healthcare during the pandemic period as: (1) in-person visits only, (2) telehealth visits only, (3) both telehealth and in-person, and (4) no visits. Propensity score matching was used to adjust for baseline characteristics.The final study sample included 25,198 patients, of whom 23,299 had a diabetes diagnosis, and 20,580 had at least one elevated A1c result.
Primary outcomes included (1) whether patients received an A1c test during the pandemic, (2) changes in A1c levels, and (3) emergency department visits and hospitalizations. The researchers examined these outcomes over two periods: March -September, 2020 and September 2020- March 2021.
The findings:
During the initial six months, patients without care had the lowest A1c testing rates (17.91%), while those with both in-person and telehealth visits had the highest (72.89%). Telehealth-only patients were more likely to receive an A1c test than in-person-only patients (57.19% vs. 47.67%), with similar trends persisting in the second period. These results indicate that telehealth played a crucial role in diabetes management during the pandemic– with those patients using telehealth more likely to receive A1c tests than those relying solely on in-person visits.
While a hybrid care model appears most effective, the significant proportion of patients who received no care highlights persistent gaps in this population. Integrating telehealth into routine diabetes management may improve access, but targeted efforts are still needed to re-engage patients who disengaged from care.
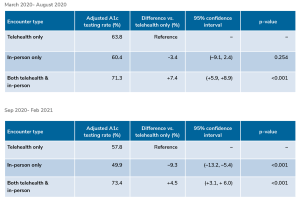
Figure titled “Patient A1c testing rates by encounter type” showing two tables that compare adjusted A1c testing rates by encounter type (Telehealth only, In-person only, Both telehealth & in-person) for patients during two time periods.
Top table (March 2020 – August 2020):
Telehealth only: Adjusted A1c testing rate 63.8% (reference).
In-person only: 60.4%; Difference vs. telehealth only: -3.4%; 95% CI (-9.1, 2.4); p-value 0.254.
Both telehealth & in-person: 71.3%; Difference +7.4%; 95% CI (+5.9, +8.9); p-value <0.001.
Bottom table (Sep 2020 – Feb 2021):
Telehealth only: Adjusted A1c testing rate 57.8% (reference).
In-person only: 49.9%; Difference: -9.3%; 95% CI (-13.2, -5.4); p-value <0.001.
Both telehealth & in-person: 73.4%; Difference +4.5%; 95% CI (+3.1, +6.0); p-value <0.001.