State telehealth reimbursement policies and hybrid perinatal care in the United States: A study of national clinical cohort collaborative data
Principal Investigator

Peiyin Hung
Associate Professor, Department of Health Services Policy and Management, University of South Carolina
Principal Investigator

Xiaoming Li
Professor, Department of Health Promotion, Education, and Behavior, University of South Carolina
Co-Investigators
- Jiani Yu, Assistant Professor, Department of Population Health Sciences, Weill Cornell Medical College
- Jihong Liu, Professor, Department of Epidemiology and Biostatistics, University of South Carolina
- Sayward Harrison, Associate Professor, Department of Psychology, University of South Carolina
- Bo Cai, Professor, Department of Epidemiology and Biostatistics, University of South Carolina
- Berry A. Cambell, Associate Professor, Department of Obstetrics and Gynecology, University of South Carolina
- Nansi Boghossian, Associate Professor, Department of Epidemiology and Biostatistics, University of South Carolina
- Adiba B. Promiti, Doctoral Candidate, Department of Epidemiology and Biostatistics, University of South Carolina
- Anirban Chatterjee, Doctoral Candidate, Department of Health Services Policy and Management, University of South Carolina
Funded By
Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD)
The problem:
Geographic disparities in access to prenatal and postpartum care persist across the United States. Telehealth has emerged as a promising modality to improve timely health care for individuals facing geographic barriers. However, the implementation of telehealth services often depends on state-level reimbursement policies. This study investigates the association between varying Medicaid telehealth reimbursement policies (asynchronous, audio-only, remote patient monitoring) and the utilization of hybrid (telehealth and in-person) versus exclusively in-person prenatal and postpartum care.
The approach:
This retrospective cohort study used nationwide electronic health records (EHR) data from June 2018 to May 2022, to examine whether a birthing individual used hybrid (telehealth and in-person) vs. exclusively in-person care before and after their residence state implemented reimbursement policies for each telehealth modality.
The findings:
The researchers found that state telehealth policies were indeed associated with increased hybrid care uptake in birthing individuals receiving prenatal or postpartum care in study health systems. State telehealth reimbursement policies provide birthing people with new options for healthcare delivery.
States seeking to promote hybrid perinatal care should consider comprehensive reimbursement policies for better integration of telehealth into perinatal care models, as robust policies have the potential to improve access and outcomes for patients facing travel burdens or geographic challenges.
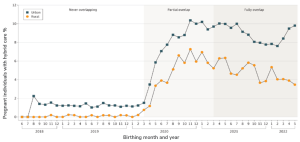
A line graph titled “Percentage of pregnant individuals with hybrid prenatal care (in-person and telehealth) from June 2018 to May 2022” depicting the percentage of pregnant individuals with hybrid prenatal care (in-person and telehealth) from June 2018 to May 2022, stratified by urban (blue squares) and rural (orange circles) residence. The x-axis shows birthing month and year; the y-axis indicates percentage (0–12%). The graph background is divided into three labeled sections: “Never overlapping,” “Partial overlap,” and “Fully overlap,” corresponding to different stages of COVID-19 pandemic exposure.
From 2018 to early 2020 (“Never overlapping”), hybrid prenatal care rates are low and stable (<2% urban, ~0% rural). During the “Partial overlap” period starting around early 2020, both urban and rural rates sharply increase: urban rates peak near 10%, and rural rates rise to about 7%. In the “Fully overlap” phase (late 2020 to 2022), rates plateau, remaining higher than pre-pandemic: urban rates fluctuate between 8% and 10%, while rural rates show more variability, between 3% and 7%. Urban rates consistently exceed rural rates throughout the period. A legend identifies urban (squares) and rural (circles) lines.
Selected Publications & Presentations
Hung, P., Granger, M., Boghossian, N., Yu, J., Harrison, S., Liu, J., Campbell, B. A., Cai, B., Liang, C., & Li, X. (2023). Dual barriers: Examining digital access and travel burdens to hospital maternity care access in the United States, 2020. The Milbank Quarterly, 1468-0009.12668. https://doi.org/10.1111/1468-0009.1266
Hung, P., Zhang, J., Chen, S., Harrison, S. E., Boghossian, N. S., & Li, X. (2024). A hidden crisis: postpartum readmissions for mental health and substance use disorders in rural and racial minority communities. American Journal of Obstetrics and Gynecology, 231(4), e117–e129. https://doi.org/10.1016/j.ajog.2024.05.047
Odahowski, C. L., Hung, P., Campbell, B. A., Liu, J., Boghossian, N. S., Chatterjee, A., Shih, Y., Norregaard, C., Cai, B., & Li, X. (2024). Rural-urban and racial differences in cesarean deliveries before and during the COVID-19 pandemic in South Carolina. Midwifery, 136, 104075. https://doi.org/10.1016/j.midw.2024.104075