COVID-19 pandemic mitigation, community economic and social vulnerability, and opioid use disorder: Updates
Principal Investigator

Elaine Hill
Professor, Departments of Public Health Sciences and Economics, University of Rochester
Principal Investigator

Meredith Adams
Associate Professor, Anesthesiology, Biomedical Informatics, Pharmacology & Physiology, and Public Health Sciences, Wake Forest University School of Medicine
Co-Investigators
- Aniket Patil, Predoctoral Research Associate, Department of Public Health and Economics, University of Rochester
- Konstantin Kunze, Postdoctoral Fellow, Department of Public Health and Economics, University of Rochester
- Grace Sventek, Predoctoral Research Associate, Department of Public Health and Economics, University of Rochester
- Daniel Guth, Postdoctoral Fellow, Department of Public Health and Economics, University of Rochester
- Sydney Pargman, Predoctoral Research Assistant, Department of Public Health and Economics, University of Rochester
Funded By
The problem:
Elaine Hill’s team set out to understand the following research questions:
- Whether the COVID-19 pandemic exacerbated the overdose crisis everywhere or whether communities with pre-pandemic vulnerability (overdose rates, unemployment) experienced the greatest burden
- If pre-pandemic and pandemic policies contributed to the overdose crisis
The approach:
Using the National Death Index (NDI) as a benchmark, Hill and her colleagues analyzed the quality of death information provided in Medicare and Medicaid enrollment files to answer the question of how accurate death data is in enrollment files.
The findings:
The team found that pre-pandemic unemployment was a key factor in the rise of opioid overdoses during the first three years of the pandemic. While its interaction with the pandemic amplified the effect, it was not fully explained by the overlap. In contrast, no comparable increases were observed for suicide or alcohol-related deaths. From a social policy standpoint, pre-pandemic policies, such as prescription limits and monitoring programs, as well as pandemic mitigation policies, did not account for these trends. Notably, counties with high pre-pandemic unemployment—not those with high pre-pandemic opioid mortality—saw the greatest increases in overall mortality.
The team found that while Medicaid enrollment files’ disagreement with the National Death Index improves over time, it still persists 5-10% in Transformed Medicaid Statistical Information System Analytic Files also known as T-MISS Analytic Files (TAF) years, however by 2010, there was over 95% Agreement for Death Dates. Additionally, the team found that the majority of state-level mortality were among beneficiaries on public insurance.
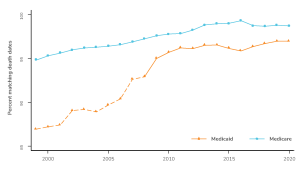
Line graph titled “Agreement of Death Date in NDI and Enrollment Files” showing percent matching death dates from 2000 to 2020 for Medicaid Decedents (red dashed line with triangles) and Medicare Decedents (light blue solid line with circles). The y-axis ranges from 85% to 100% matching. The light blue line (Medicare Decedents) starts near 95% in 2000 and rises gradually to about 98% by 2015, remaining steady through 2020. The red line (Medicaid Decedents) starts at about 87% in 2000, increases steadily, and closes the gap over time, reaching about 95% by 2015 and staying steady through 2020.
Selected Publications & Presentations
Hill, E., Mehta, H., Sharma, S., Mane, K., Xie, C., Cathey, E., Loomba, J., Russell, S., Spratt, H., DeWitt, P. E., Ammar, N., Madlock-Brown, C., Brown, D., McMurry, J. A., Chute, C. G., Haendel, M. A., Moffitt, R., Pfaff, E. R., Bennett, T. D., & the RECOVER Consortium. (2022). Risk Factors Associated with Post-Acute Sequelae of SARS-CoV-2 in an EHR Cohort: A National COVID Cohort Collaborative (N3C) Analysis as part of the NIH RECOVER program [Preprint]. Infectious Diseases (except HIV/AIDS). https://doi.org/10.1101/2022.08.15.22278603